US Pharmacopoeia Cannabis — 19th-C Medicine, 1850-1942
For ninety-two years cannabis was a mainstream Western medicine — listed in the USP, manufactured by Parke-Davis and Eli Lilly, sold in patent cough syrups and asthma cigarettes. Then they removed it.
The pharmacopoeia story is the most inconvenient fact in the entire prohibition narrative. For nearly a century, cannabis was not a fringe remedy or an underground curiosity. It was a recognized medicine, listed in the official drug compendia of multiple Western nations, manufactured by the most respected pharmaceutical firms in the world, and prescribed by physicians for conditions ranging from migraines to menstrual cramps. When Congress criminalized it in 1937, it did so over the explicit objection of the American Medical Association.
Entry into the USP
Cannabis enters the United States Pharmacopoeia
The third edition of the USP lists Extractum Cannabis as an official medicine. It will remain through the eleventh revision.
The United States Pharmacopoeia first admitted cannabis in 1850, in the third edition, under the name Extractum Cannabis. This was just eleven years after O'Shaughnessy's landmark paper in Calcutta — a remarkably fast adoption by the standards of nineteenth-century medicine. Cannabis remained in successive editions through the eleventh revision.
Cannabis removed from the USP
The twelfth edition of the United States Pharmacopoeia drops cannabis — five years after the Marihuana Tax Act made its legal prescription essentially impossible.
The twelfth edition removed cannabis in 1942, five years after the Marihuana Tax Act had made legal prescription effectively impossible. The removal was administrative, not pharmacological — cannabis did not suddenly stop working in 1942. It became too legally cumbersome for physicians to prescribe.
The British Pharmacopoeia followed a parallel trajectory, listing cannabis from the 1860s until 1932.
The pharmaceutical manufacturers
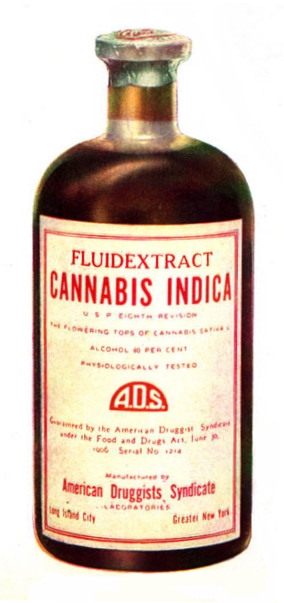
Cannabis was not a cottage-industry product. A remarkable cluster of America's and Europe's most prominent pharmaceutical firms produced cannabis preparations throughout the second half of the nineteenth century and into the twentieth:
- Tilden & Company of New Lebanon, New York — whose cannabis extract was the drug of choice for the literary experimenters of the 1850s, including Fitz Hugh Ludlow.
- Parke-Davis of Detroit, which in the 1890s collaborated with Eli Lilly to breed a standardized strain called "Cannabis Americana" grown on Indiana farms and sold into the 1930s.
- E.R. Squibb & Sons, whose name survives in modern Bristol-Myers Squibb.
- Burroughs Wellcome, the British firm whose legacy continues as GlaxoSmithKline.
- Merck, already one of the largest pharmaceutical companies in the world.
- Grimault & Cie of Paris, whose "Cigarettes Indiennes de Cannabis Indica" were marketed internationally as an asthma remedy and advertised in American newspapers from 1876 onward.
By the 1930s, roughly 280 American manufacturers produced more than 2,000 cannabis-containing medicines. These were not marginal products. They were sold by the same companies that manufactured aspirin, quinine, and morphine — the mainstream pharmacopoeia of the era.
Patent medicines and the pre-regulation era
Before the Pure Food and Drug Act of 1906 required ingredient labeling, cannabis was — after alcohol and opium — reportedly the third most common active ingredient in American patent medicines. Consumers often had no idea what they were taking. Specific products whose cannabis content is documented include:
- Piso's Cure for Consumption (Hazeltine & Co., Warren, Pennsylvania, from 1864) — which blended cannabis indica with chloroform, alcohol, and originally morphine. Samuel Hopkins Adams attacked it in his 1905 Collier's Weekly exposé series The Great American Fraud.
- Kohler's One Night Cough Cure, documented by the U.S. Government in Kebler's Habit-Forming Agents (1910).
- Dr. J. Collis Browne's Chlorodyne, a British preparation widely available in America.
- Gunjah-Wallah Company's maple-syrup hashish candies, advertised in Vanity Fair as a confection.
The 1906 Pure Food and Drug Act did not ban cannabis. It required that products containing cannabis (along with alcohol, morphine, cocaine, and other substances) be labeled accurately. The act reflected Progressive Era consumer-protection values, not anti-drug panic. Cannabis was treated as a medicine that required disclosure, not as a narcotic that required suppression.
The Queen Victoria myth
The Queen Victoria story appears to have been fabricated or exaggerated in 1970s pro-cannabis literature. Even Ethan Russo, a respected cannabis researcher who once endorsed the anecdote, now characterizes it as unsubstantiated. Reynolds was Victoria's physician from 1878; Reynolds did advocate cannabis for dysmenorrhea in the Lancet. But the leap from "her physician recommended cannabis for menstrual pain" to "he prescribed it to the Queen" requires evidence that does not exist.
This matters because the claim is deployed as an argument from authority — if the Queen of England used it, surely it must be legitimate. The actual evidence for cannabis's nineteenth-century medical legitimacy is overwhelming and does not require a royal endorsement. Cite the Reynolds paper with confidence. Cite the Queen Victoria anecdote not at all, except to debunk it.
The standardization problem
Cannabis had a genuine pharmaceutical weakness that its competitors — morphine, chloral hydrate, and eventually aspirin — did not share: inconsistent potency. Different batches of plant material, grown in different climates and harvested at different stages, produced wildly variable concentrations of active compounds. Physicians could not reliably predict dosing, which made cannabis less convenient than alternatives whose active ingredients could be isolated and measured.
This was not a fatal flaw — physicians worked around it for decades. But it made cannabis vulnerable to displacement by drugs with more predictable pharmacology, particularly after the synthesis of barbiturates (1903) and aspirin's mass-market success. The Marihuana Tax Act of 1937 did not kill a thriving pharmaceutical market; it killed a declining but still significant one.
The arc of legitimate medicine
The pharmacopoeia record establishes a simple, documented fact that no amount of prohibitionist rhetoric can erase: for ninety-two years, from 1850 to 1942, cannabis was an official medicine in the United States. It was manufactured by firms whose corporate descendants remain among the world's largest pharmaceutical companies. It was prescribed by licensed physicians for recognized medical conditions. And it was removed not because new evidence demonstrated it was dangerous or ineffective, but because a tax act made it legally impractical to prescribe.
When modern advocates argue that cannabis has "no accepted medical use" — the language of Schedule I — the pharmacopoeia record is the first and most devastating rebuttal. Western medicine accepted cannabis for nearly a century. Then it chose to forget.
For in-depth cannabis education, dosing guides, safety information, and research summaries, visit our partner site TryCannabis.org